The Psychological Impact of Prostate‑Related Conditions: A Scientific Overview
IntroductionProstate‑related disorders—such as benign prostatic hyperplasia (BPH), prostatitis, and prostate cancer—affect millions of men worldwide. While clinical discussions often focus on urinary symptoms and cancer‑specific markers, a growing body of evidence highlights the strong bidirectional relationship between prostate health and mental health. Psychological factors such as anxiety, depression, and stress can both influence the onset and severity of prostate symptoms, and conversely, prostate disease can significantly impair emotional well‑being, sexual function, and overall quality of life.
Psychological Effects of Benign Prostatic Hyperplasia (BPH)Benign prostatic enlargement commonly causes lower urinary tract symptoms (LUTS), including urgency, frequency, nocturia, and weak stream. These symptoms not only disrupt sleep and daily activities but also have a measurable impact on mood and social functioning.Anxiety and embarrassment: Men with BPH often experience anxiety about “losing control” of urination in public, leading to avoidance of social events, travel, and workplaces. This social withdrawal can foster feelings of shame, low self‑worth, and chronic stress.
Depression and self‑esteem: Persistent nocturia and daytime fatigue can contribute to mild‑to‑moderate depression and a sense of inadequacy, especially when urinary symptoms interfere with work performance or intimate relationships. Epidemiological studies show that men with symptomatic BPH report higher rates of anxiety, depression, and somatization compared with age‑matched controls, suggesting that treatment of LUTS must include attention to psychological status.
Prostatitis and Mental Health
Chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS) is a particularly vexing condition because symptoms may persist for years and respond poorly to standard therapies.
Stress as a trigger and amplifier: Psychological stress has been associated with worsening pelvic pain, urinary discomfort, and sexual dysfunction in prostatitis patients. Elevated cortisol and autonomic nervous system arousal may increase pelvic muscle tension and local inflammation, intensifying pain signals.
Hopelessness and emotional burden: Because CP/CPPS is often difficult to diagnose and treat, patients may feel “doomed” or misunderstood, leading to hopelessness, irritability, and secondary depression.
Psychological support, cognitive‑behavioral techniques, and sometimes pharmacotherapy are increasingly recommended as part of a multidisciplinary approach to chronic prostatitis.
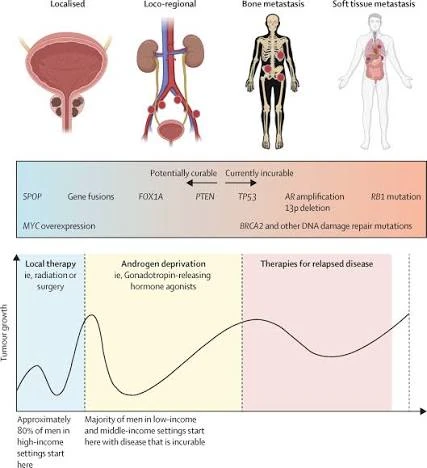
Prostate Cancer, Anxiety, and DepressionProstate cancer is one of the most common malignancies in men, and its diagnosis carries a substantial psychological load.Anxiety and uncertainty: Men diagnosed with prostate cancer frequently experience anxiety related to survival, treatment side‑effects, and the possibility of recurrence. Concerns about rising PSA levels or new imaging results can trigger chronic worry, often independent of actual disease progression.
Depression and stigma: Studies report that anxiety affects up to one‑third of prostate cancer patients, while depression is present in roughly 12–15% of this group. Side‑effects such as sexual dysfunction, urinary incontinence, and hormonal changes (e.g., androgen‑deprivation therapy) can further damage body image, self‑esteem, and intimacy, increasing vulnerability to mood disorders.
Support groups, counseling, and survivor‑wellness programs have been shown to reduce symptom burden and improve emotional adjustment for men living with prostate cancer.
Bidirectional Pathways and Management ImplicationsThe relationship between the prostate and the psyche appears to be bidirectional:Mental disorders, smoking, and alcoholism are more common in men seeking prostate assessments, and those with uncured benign prostate disease show higher levels of anxiety, depression, and psychosis at follow‑up.
Inflammatory and neuroendocrine pathways—such as activation of the sympathetic nervous system, cortisol release, and alterations in serotonin and norepinephrine—may link psychological stress to enhanced LUTS and pelvic pain.
Clinically, this calls for a holistic model that integrates urological treatment with mental‑health screening and support. Routine assessment of depression and anxiety using brief tools (e.g., PHQ‑9, GAD‑7), alongside prostate‑specific questionnaires, allows early identification of at‑risk patients and timely referral to psychologists or psychiatrists.
Conclusion
Prostate‑related conditions are not isolated urological or oncological problems; they are deeply intertwined with a man’s psychological state. Anxiety, depression, and chronic stress can both worsen prostate symptoms and emerge as consequences of these diseases. Addressing mental health within prostate care—through counseling, lifestyle modification, and appropriate medications—can improve symptom control, enhance treatment adherence, and restore a sense of agency and well‑being in affected men. Future research should continue to explore the neurobiological links between the prostate and the brain, and to refine integrated care pathways that treat both the body and the mind.